| Colonic Fibrovascular Polyp |
The original report was published in J Gastroenterol 1994;29:763-766.
Abstract A case of a fibrovascular polyp of the sigmoid
colon is reported. The patient tested positively
for fecal occult blood on a mass survey for
colorectal cancer, and underwent colonoscopic
examination which revealed a pedunculated
submucosal tumor in the sigmoid colon. The
tumor, about 10mm in diameter, had a short
thin stalk and was removed endoscopically;
the histological diagnosis was fibrovascular
polyp. This extremely rare polyp is discussed,
and particular attention is focused on the
unusual endoscopic features and on the appropriate
management.
a Higashi Kanamachi Naika Clinic, 7-5-8-1
Higashi Kanamachi, Katsushika, Tokyo 125-0041,
Japan. We recently encountered a case of colonic
fibrovascular polyp that showed characteristic
endoscopic features. Fibrovascular polyps,
which are pedunculated submucosal tumors,
are occasionally found in the esophagus,[1-8] but are extremely rare in the colon. The
present report focuses on the diagnostic
problems and on appropriate management. A 72-year-old Japanese woman was referred
to Mutsu General Hospital in Aomori Prefecture
in August 1991 for follow up of positive
fecal occult blood test (determined by reverse
passive hemagglutination) conducted in a
mass survey for colorectal cancer. She had
no complaints and had had no changes in bowel
habits. She was given a barium enema, which
showed a polyp, about 1cm in diameter, in
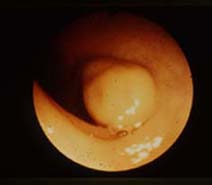
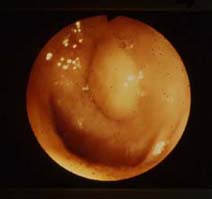
the sigmoid colon(Figs. 1,2). Subsequent colonoscopy revealed that the
polyp was pedunculated and not ulcerated,
and had a smooth surface, with the same color
as the surrounding mucosa; the mucosa around
the tumor appeared normal(Figs. 3,4). The polyp was elastic and easily indented
by biopsy forceps(Fig. 5), but it did not spring back to its previous
shape immediately after the biopsy forceps
was opened. The biopsy specimens taken from
its distal end showed normal colonic mucosa.
The patient did not have an elevated sedimentation
rate or eosinophilia. Upper gastrointestinal
endoscopy revealed that the patient also
had a duodenal ulcer. A tentative diagnosis
of submucosal tumor was made and the tumor
was endoscopically polypectomized, using
a diathermy snare, with no complications
such as perforation or hemorrhage occurring.
It took time to excise the polyp. The excised
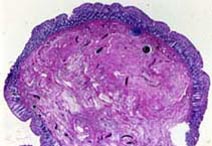
polyp was 9x4x11mm in size. Histologically,
the tumor consisted of fibrous tissue containing
blood vessels and lymphatics; it was completely
covered by normal colonic mucosa and by the
muscularis mucosae(Fig. 6), but it contained a little blood. The mucosa
covering the tumor was 0.6mm in thickness
and had no vascular proliferation. The microscopic
appearance was similar to that of a fibrovascular
polyp of the esophagus. The fibrous core
was stained blue with Azan stain, and blue
violet with Weigert's fibrin stain, but did
not stain blue with phosphotungstic acid
hematoxylin(PTAH)stain. The patient had a
favorable course and a barium enema 5 months
later showed no recurrence. In one study,[9] a total of 376 cases of submucosal tumors
of the large bowel were reported; 127 cases(34%)were
benign tumors, including 47 leiomyomas, 42
lipomas, 11 lymphangiomas, and 10 hemangiomas.
The other 249 cases were malignant submucosal
tumors, and these constituted 1.3% of all
cancers of the colon and the rectum.[9] Up to 80 cases of fibrovascular polyps
of the esophagus have been reported; [1-8,17] however, we found no reports of a colonic
fibrovascular polyp. The gross endoscopic impression is heavily
relied on in making a diagnosis. Because
nonepithelial tumors are usually covered
by normal mucosa, most of them are easily
distinguishable from epithelial tumors. Some
submucosal tumors, such as lipomas, lymphangiomas,
and hemangiomas, have endoscopically characteristic
findings.[10-15] Lipomas and lymphangiomas are smooth and
softer than other tumors. Lipomas can usually
be indented with closed biopsy forceps and
tend to spring back rapidly to their previous
shape upon withdrawal of the forceps, this
being known as the "pillow," "cushion,"
or "tenting sign".[10,11] After the mucosa covering a lipoma is removed
by the taking of multiple biopsies, fat can
be seen protruding from the biopsy site;
this is called the "naked fat sign."[12] Lymphangioma occurs as a fluctuant and
cystic mass;[13] peristalsis, compression, and the patient's
position changes its shape.[14] After the surface mucosa is removed, serous
and clear liquid usually flow out from the
biopsy site and its size is then reduced.[14] Most hemangiomas show endoscopically characteristic
findings of small bluish discolorations or
bright cherry-red spots.[15] The fibrovascular polyp seen in our patient
did not have the above characteristic findings.
It is thought to be characteristic that this
tumor was easily depressed when grasped with
biopsy forceps, and it did not spring back
rapidly to its previous shape. The authors
believed that the biopsy forceps had extruded
the blood and lymph fluid from the fibrovascular
polyp, causing the polyp not to spring back
to its original shape. Usually it takes time
to excise a submucosal tumor, because it
is necessary to cut its muscularis mucosae. Fibrovascular polyps are benign submucosal
tumors, and are covered by normal mucosa
that may be focally ulcerated. Histologically,
these tumors consist of spindle cells, occasionally
arranged in whorls, and loose vascular connective
tissue. In such tumors of the esophagus,
mononuclear cell infiltration varies from
minimal to severe, and tends to be prominent
distally; however, the present tumor showed
only minimal chronic inflammation. Histological
differential diagnosis is with other mesenchymal
tumors, including fibromas, leiomyomas, and
inflammatory fibroid polyps; the present
tumor was not reminiscent of these tumors
because of the lack of common histological
features. The fibrous core was stained blue
with Azan stain, indicating collagen fibers;
the findings of PTAH staining indicated that
this core did not consist of fibrin or fibrinoid
as the result of congestion.
Rigorous histopathological examination is
necessary to differentiate a fibrovascular
polyp from the congestion and chronic inflammation
resulting from idiopathic intussusception
in the ileocecal area;[16] the polyp found in the present patient
showed submucosal fibrovascular proliferation
rather than simple congestion, and was accompanied
by few inflammatory cells, without a whorl
arrangement of stromal cells around vessels. Lodmell[17] reported a patient with fibrovascular polyp
of the esophagus whose presurgical laboratory
findings showed eosinophilia and an elevated
sedimentation rate; these findings were not
shown in our patient. The propulsive forces created by peristalsis,
combined with the traction of the passing
stool must lead, in the sigmoid colon, to
the development of a pedunculated structure.
Although it is possible that the fibrovascular
polyp reported here was a secondary change
of the submucosal fibrovascular tissue, its
histogenesis is unclear.
The clinical manifestations of submucosal
tumors of the colon are related to their
size, and large submucosal tumors may cause
intussusception. Like fibrovascular polyps
of the esophagus, those of the colon may
become large. This suggests that a fibrovascular
polyp of the colon has the potential to cause
intussusception. Most fibrovascular polyps
of the esophagus are large and vascular;
the routine removal of fibrovascular polyps
of the esophagus is controversial. Patel
et al.[2] reported one in which the length was 17cm
and which had large vessels running throughout
its core; they elected surgical excision.
Siddins and Cade,[8] however, reported a case of a smaller fibrovascular
polyp of the esophagus, 10cm in length, which
was safely removed endoscopically. Diathermy
polypectomy is not always dangerous in resecting
smaller fibrovascular polyps of the esophagus.
In the present patient, because of the polyp's
small size and thin stalk, colonoscopic polypectomy
was undertaken with adequate hemostasis,
and the polyp was found to contain relatively
few blood vessels histologically. If small
fibrovascular polyps of the colon grow slowly,
similar to those of the esophagus, it is
necessary to remove them safely endoscopically
before they grow, increase in vascularity
and cause intussusception. Since, to our knowledge, this is the first
lesion of this kind ever encountered, it
is obvious that there is no way to make an
accurate diagnosis for polypectomy. Although
the surgical resection of a submucosal tumor
is usually undertaken due to its submucosal
location,[18,19] polypectomy for a pedunculated submucosal
tumor is a reasonable method when the tumor
does not have features of hemangioma, because
one can expect both exact histopathological
diagnosis and complete resection, and the
procedure is less harmful for the colonic
wall. Accurate endoscopic diagnosis of submucosal
tumors is difficult. In the series cited
above, 249 of 376 submucosal tumors, 66%
were shown to be malignant.[9] References
b Second Department of Pathology, Hirosaki
University School of Medicine, 5 Zaifucho,
Hirosaki, Aomori 036-8562, Japan.
Introduction
Case report



Discussion
The original report was published in
J Gastroenterol
1994;29:763-766.